
Almost never with modern grafting.
This is a question that comes to us at Lema Dental Clinic every single day. A patient, most likely around 60 or 70 years old, looks at the gap in their smile that they have been hiding for years and asks, “Is the door closed for me? Have I waited too long to come?”
The short answer is: No.
However, the long answer is interesting because it doesn’t involve time on a clock. It is about biology.
Here in Turkey, in our clinical practice, we see that patients mix up age with bone capacity quite often. They come to believe that because the tooth was lost ten years ago, the jawbone is gone for good. The truth is more complex. The bone does resorb, similar to a shoreline that is washed away over time without a sea wall, but with the help of modern surgery, we can rebuild that shore for a dental implant.
The Foundation Analogy: Why Bone Is More Important Than Age
Imagine the scenario when you plan to hammer a nail into a wall. If the drywall is sturdy and thick enough, the nail will easily hold the picture frame. Conversely, if the wall is too thin or has been damaged, the nail won’t be able to grip anything.
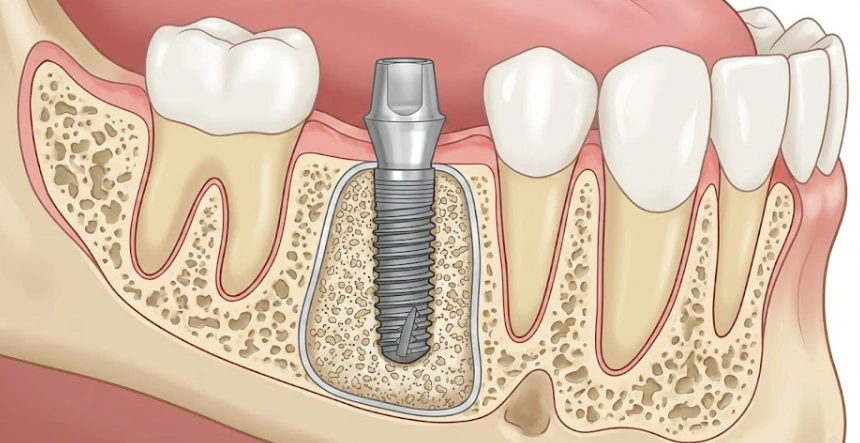
Implants in the oral cavity are analogous to nails. The titanium implant is the nail; the bone is the wall.
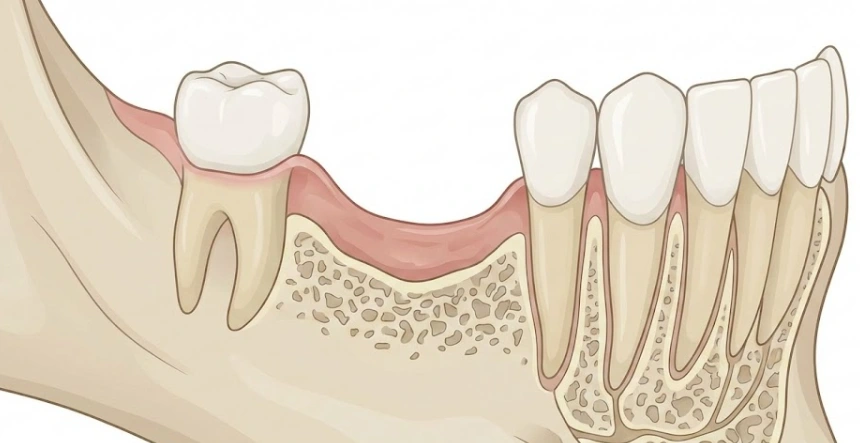
Once the tooth is lost, the brain sends a signal that it will no longer support that particular area of the jaw. It initiates the process of resorption. The body is smart to recycle that bone mineral into somewhere else where it might be more useful.
Nonetheless, a thinner base does not necessarily mean that one can’t strengthen it. Professor Doctor Coşkun Yıldız, a well-known maxillofacial surgeon in the country, insists on his patients’ hearing: “We are not merely placing teeth; we are the architects of the jaw.” There is still a possibility to create a brand new foundation even if the natural one is a bit weak.
The Cases When “Too Late” Means Just “More Complex”
It is usually very hard to find any situations when Lema Dental Clinic would completely refuse to give implants to a patient who had their implants previously removed. What happens is that the dialogue becomes more about reconstructing the jaw than about carrying out a routine operation.
Let us assume that you have delayed the treatment for years, then the following chain of events usually occur:
- Biting Bone Loss with a decrease in height: The jawbone height gets reduced.
- Facial Bone Loss with a decrease in width: The width of the ridge gets narrowed.
- Sinus Enlargement: The air cavity (sinus) in the upper jaw descends due to the absence of tooth roots supporting it.
These would be considered red flags by a green dentist, while to Dentist Polen Akkılıç and her staff, these are merely obstacles that, by following the right procedures, we rise over.
[twenty20 img1=”375039″ img2=”375021″ direction=”horizontal” offset=”0.5″ align=”right” width=”50%” before=”Before” after=”After” hover=”true”]The Arsenal for “Hopeless” Situations
If you have been told that you have “inadequate bone,” it mostly means that you need one of the following before the implant is inserted:
- Guided Bone Regeneration (GBR): The jawbone ridge is enlarged by the use of bone graft materials (synthetic, bovine or your own). Just like a pillar that is reinforced with fresh concrete and rebar before the construction of the second floor.
- Sinus Lifting: This procedure is related to the upper jaw only. The sinus membrane is lifted by a small amount and bone is packed underneath it. In this way, an implant cannot poke into the sinus cavity because a safe “floor” has been created by the bone.
- Zygomatic Implants. This is the absolute answer in the case of severe bone loss where even grafting is not an option. The implants are longer and they do not even touch the jawbone as they are anchored to the cheekbone (zygoma). This is the kind of operation that Professor Doctor Coşkun Yıldız is really good at and it is a great thing that he rarely has to allow patients to be his permanent denture example.
Most of the Time It Isn’t The Calendar
So, what is then, if time is not the enemy?
It is when a line in the medical chart stands out in a way that makes carrying out the procedure impossible. The patient could have an uncontrolled, active gum disease (periodontitis), which would be a red flag of the highest order—it’d be like building a house in the middle of a swamp. The infection needs to be eliminated first.
Furthermore, individuals who are on high-dose IV bisphosphonates, usually a cancer medication, or who have undergone radiation therapy of the jaw recently have an increased risk for developing osteonecrosis. In such medical backgrounds, we take a break. But when it comes to a fit and healthy 80-year-old who has got a gap for 20 years? We do implants in such situations without any problem all the time.
Your Choices At A Glance: Timelines And Expectations
Let’s see how the procedure will be affected by waiting. The longer a tooth is missing, the more likely it is that additional steps will be required.
| Scenario | Bone Condition | Likely Procedure | Estimated Timeline (Turkey) |
| Tooth lost < 6 months ago | High density, good volume. | Immediate/Standard Implant | 1 Visit (or 2 visits 3 months apart). |
| Tooth lost 2-5 years ago | Moderate resorption (width loss). | Implant + Minor Bone Graft | 2 Visits (3-4 months healing). |
| Tooth lost 10+ years ago | Severe resorption (height & width). | Sinus Lift / Block Graft | 2 Visits (6 months healing for graft). |
| Complete Edentulism (decades) | “Paper thin” jawbone. | All-on-4 or Zygomatic Implants | Variable (often immediate fixed teeth). |
Top Concerns About Delayed Implant Treatment
Yes, in most cases. Osteoporosis affects the density of long bones (like hips) more severely than the jaw. However, it does change how we approach the surgery. Dentist Polen Akkılıç may recommend a longer healing period (osseointegration) to ensure the implant fuses solidly with the bone before we place the final crown. We treat osteoporosis patients at Lema Dental Clinic regularly with high success rates.
Not necessarily. The placement of the implant itself is generally not painful due to local anesthesia. However, if you require extensive bone grafting or a sinus lift because of the delay, the post-operative swelling might be slightly more pronounced than a standard case. We manage this with advanced medication protocols to keep you comfortable.
Aesthetics are our obsession. The challenge with long-term tooth loss is that the gum line recedes along with the bone. If we just placed a tooth there, it might look “long.” To counter this, we use pink porcelain or composite at the base of the crown to mimic healthy gum tissue, or we perform soft tissue grafting. The result is a seamless blend.
Healing slows down slightly as we age, but the mouth is incredibly resilient. We have successfully treated patients in their late 80s. The primary requirement is not “youth” but general health. If you are healthy enough to undergo a minor tooth extraction, you are generally healthy enough for an implant.
When you are dealing with “late-stage” restoration involving sinus lifts or zygomatic implants, expertise matters. Turkey, and specifically Lema Dental Clinic, has become a global hub for these complex surgeries because of the high volume of cases we handle. Professor Doctor Coşkun Yıldız sees more complex bone structures in a month than many general dentists see in a career. Plus, the cost-efficiency allows you to access premium Swiss or German implant brands that might be cost-prohibitive elsewhere.
- Buser, D., Sennerby, L., & De Bruyn, H. (2017). Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontology 2000, 73(1), 7-21.
- Chappuis, V., Araujo, M. G., & Buser, D. (2017). Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000, 73(1), 73-83.
- Esposito, M., Grusovin, M. G., & Worthington, H. V. (2013). Interventions for replacing missing teeth: Treatment of periodontitis and other gum diseases to improve implant outcomes. Cochrane Database of Systematic Reviews, (3).
- Misch, C. E. (2007). Contemporary Implant Dentistry. Mosby Elsevier.
- Aparicio, C., Manresa, C., Francisco, K., & Ouazzani, W. (2014). Zygomatic implants: indications, techniques and outcomes, and the zygomatic success code. Periodontology 2000, 66(1), 41-58.

