
Yes, sinus pressure mimics tooth pain.
This is a scenario that we witness frequently, especially in allergy season or the winter period. There comes a patient, who firmly believes that the only cure for them is an emergency root canal, to our clinic in Istanbul. The upper back teeth continue to be the source of pain, the pain is unbearable, and the patient is almost ready in their mind for dental surgery.
However, quite often after we have done a clinical examination and taken digital X-rays, we have to tell them the shocking reality: You don’t have any dental problems at all. It is your sinuses that are giving you the pain.
Actually, the link between your nose and your mouth is much closer than most people would think.
The principle at Lema Dental Clinic, which is largely Professor Doctor Coşkun Yıldız-driven, is that we never carry out dental treatment unless we are sure that the tooth is the cause of the pain. Recognizing the biological convergence of sinusitis and dental problems is important for preventing unnecessary treatments.
We explain here why this is the case and how you can tell whether it is a dental emergency or just a bad head cold.
The Anatomy of a “False” Toothache
What is the cause of the pain in your molars if you have a nasal infection? It is all down to simple geographical factors.
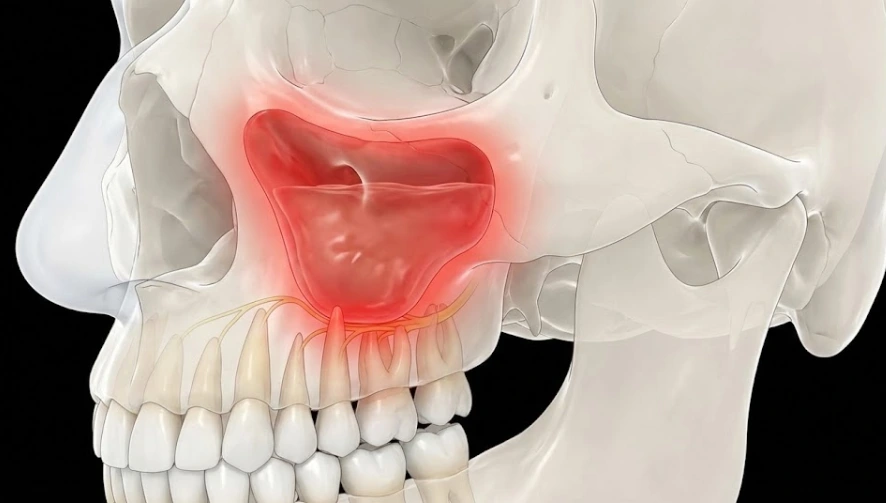
Maxillary sinuses are the largest among the paranasal sinuses and occupy the body of the maxilla (cheekbone). They are part of the facial bones and are located laterally on both sides of the nose. The palatine process of the maxilla makes their floor, which is also the area of the roots of the upper molar and premolar teeth. The roots of your upper molars and premolars are quite close to, or in some cases even protruding into, the floor of the maxillary sinus.
You can picture the roots of your teeth as a chandelier hanging in the living room downstairs, while your sinuses as the floorboards of the bedroom upstairs. For a great number of patients, the bone between these two places is so thin that it is almost like a piece of paper. In some instances, portions of the root protrude into the sinus cavity.
When the sinus cavities become inflamed and full of mucus, the pressure accumulates, and the nerve endings of the tooth roots that are closest to the sinus cavity are the first ones to be compressed by this pressure.
You do recognize the sensation as tooth pain, but it is not the case of the pressure from the tooth going into the brain. Hence, the brain is tricked by the signals and localizes the pain in the tooth even though the real cause is the sinus inflammation and the nerve endings being pressed.
How to Tell the Difference (The Diagnostic Checklist)
In reality, only professional diagnostics performed with 3D imaging here in Turkey can guarantee the absolute certainty of the situation. However, some clear signs may help you “decode” the nature of your “sinus toothache”.
Dentist Polen Akkılıç and her clinical team have successfully helped many patients with their pain issues by using a simple checklist to determine the source of pain.
The Movement Test
This one can be the most effective. For instance, when you are about to tie your shoes or walk downstairs, does the pain increase? Since sinus pain is positional, as your movement causes the fluid in your head to shift, the pressure there rises. On the other hand, dental pain from a dying nerve persists regardless of your head position.
The “Neighborhood” Effect
An abscessed or decayed tooth problem is very much on its own- it inflicts severe pain on one specific tooth. On the other hand, pain caused by the sinuses does not generally present itself in only one tooth. Usually, a patient experiences a dull ache and pressure in the vicinity of several teeth in the upper back area on one or both sides.
Associated Symptoms
Are your teeth the only things causing you discomfort? If in addition to having tooth pain you also have symptoms such as a runny nose, nasal congestion, headache behind the eyes, or low-grade fever, then the primary issue is probably respiratory rather than dental.
Comparing Symptoms: Dental vs. Sinus Origin
Before traveling to Turkey for treatment, we show our patients the symptoms explained in a simple chart format to help them better recognize their issues.
| Feature | True Dental Pain (Cavity/Abscess) | Sinus-Referred Tooth Pain |
| Location | Usually isolated to a single, specific tooth. | Diffuse pain across multiple upper back teeth. |
| Nature of Pain | Sharp, stabbing, or intense throbbing. | Dull, constant ache or feeling of heavy pressure. |
| Temperature Sensitivity | Extreme, lingering pain to hot or cold drinks. | Usually minimal to none. |
| Effect of Movement | Pain level stays relatively consistent. | Pain worsens significantly when bending over or jumping. |
| Other Symptoms | Swollen gums, bad taste in the mouth. | Congestion, headache, post-nasal drip, fever. |
The Lema Approach: Diagnosis Before Drilling
We understand that pain is pain. Whether it stems from a sinus infection or a dying nerve, it is debilitating and requires attention.
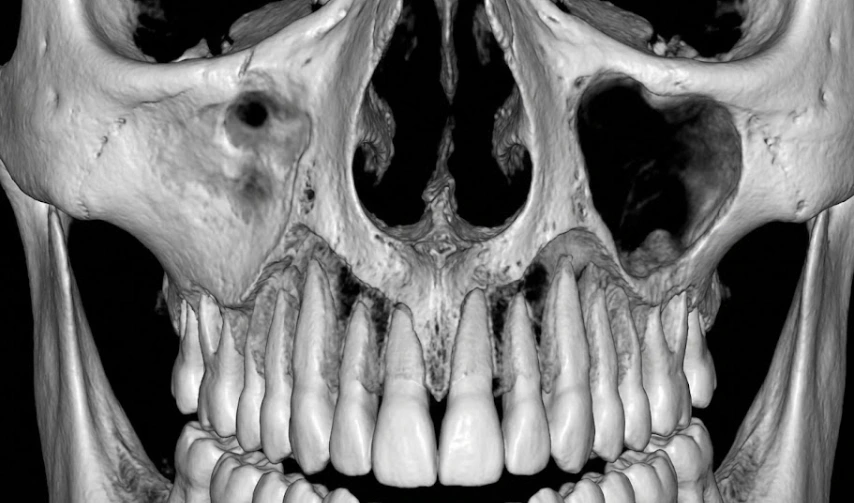
When international patients contact Lema Dental Clinic with these ambiguous symptoms, we don’t rush to book them for veneers or implants. Our first step is always accurate diagnostics using advanced Cone Beam CT scanning at our Istanbul facility. This technology allows us to see the teeth, bone, and sinus cavities in three dimensions.
If Professor Doctor Yıldız determines the issue is purely sinus-related, we will ethically refuse to perform dental work and refer you to an Ear, Nose, and Throat (ENT) specialist and recommend decongestants or antibiotics. However, if the scan reveals a dental abscess that has caused a secondary sinus infection (which also happens!), we can treat the root cause immediately.
Don’t guess with your health. If you have persistent upper tooth pain, get it checked by professionals who look at the whole picture.
FAQ: Your Questions Answered by the Experts
Almost exclusively the upper back teeth—your molars and premolars. The roots of lower teeth and front upper teeth are generally too far away from the maxillary sinuses to be affected by sinus pressure.
The tooth pain will last exactly as long as the sinus inflammation lasts. Once the infection clears, the mucus drains, and the pressure is relieved, the toothache should disappear completely. If the sinus infection resolves but the tooth pain remains, you likely have a separate dental issue that needs attention here in Turkey.
Sometimes, but it’s complicated. The broad-spectrum antibiotics often prescribed for sinusitis might temporarily knock back a dental infection, providing short-term relief. However, they rarely cure a deep tooth abscess. You should never rely on leftover sinus medication to treat dental pain; it requires a dentist’s assessment.
This is a very common frustration. If your dentist finds no decay and your X-rays are clear, it is highly probable that the issue is referred pain from sinuses or perhaps tooth grinding (bruxism). We recommend seeing an ENT specialist next.
Flying with active, severe sinus congestion can be extremely painful due to cabin pressure changes during takeoff and landing. It can also exacerbate the pressure on your teeth. We strongly advise patients to ensure their acute sinus infection is managed by a doctor before boarding a flight for dental treatment.
- American Association of Endodontists. (2018). Maxillary Sinusitis of Endodontic Origin. Endodontics: Colleagues for Excellence.
- Figueiredo, R., et al. (2021). Differential diagnosis of temporomandibular joint disorders and other orofacial pain conditions. Journal of Oral Rehabilitation, 48(12), 1349-1362.
- Little, R. E., et al. (2020). Rhinosinusitis and the Dentist: The Role of Dental Practitioners in Diagnosis and Management. British Dental Journal, 228(6), 453-458.
- Renton, T. (2019). Dental Pain related to non-dental conditions. Dental Update, 46(5), 420-430.
- Tatli, U., et al. (2022). Anatomical Relationship between the Roots of Maxillary Posterior Teeth and the Sinus Floor: A Cone Beam CT Study. Journal of Clinical and Experimental Dentistry, 14(2), e147–e154.

