
High-quality veneers don’t smell.
That is basically an unspoken concern that a lot of patients have before they book their flights to Turkey. You wish for a Hollywood smile with all the brightness and perfect symmetry. But you definitely don’t want to experience the “veneer breath” that you have read about on forums.
Here’s the truth: porcelain veneers themselves can’t actually produce an odor. It’s because they are a solid, non-porous ceramic material. So, they can’t absorb odors the way natural teeth or composite resins might.
Then, why is it that some folks report having a foul smell after getting a new set of teeth?
According to our clinical work at Lema Dental Clinic, we have never blamed porcelain as the problem. Almost in all cases, it is the biology surrounding porcelain that is the issue. We will go into details on the reasons why it happens and what Dentist Polen Akkılıç with her team have done to make sure that you won’t have to experience it.
The “Ledge” Effect: Where Bacteria Hide
Think about this scenario: you are trying to find space for another book in a jam-packed shelf. If the book isn’t perfectly in line, it’ll be a bit of a protrusion and a tiny gap will be left for dust to accumulate.
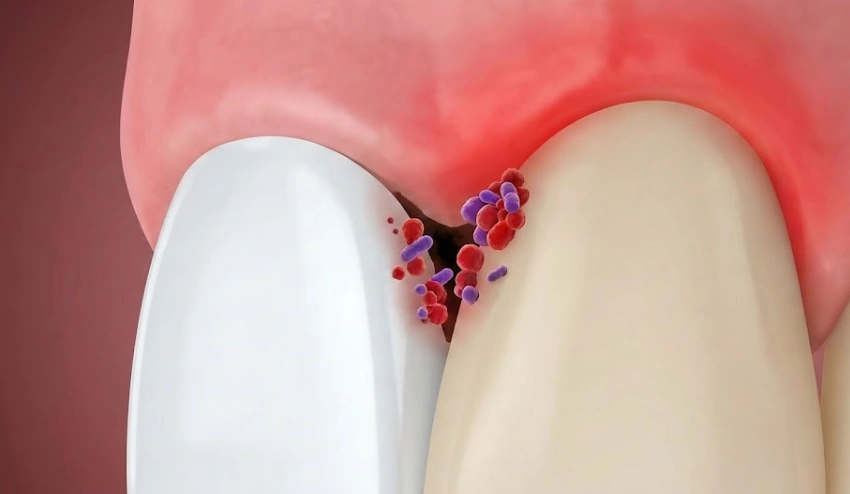
It’s the same with dental veneers. If a veneer is not bonded to the tooth with microscopic precision, it creates a “ledge” or a margin gap. A bad odor is the major symptom of such gap.
Food and bacteria love these ledges. They sneak into this tiny space between the dental porcelain and the natural tooth structure. Your toothbrush can’t reach inside the gaps because it is too big, and even floss slides over it without cleaning . Gradually, this debris thrown inside begins to ferment. There you have the smell.
At our clinic in Istanbul, we often hear patients from other clinics asking if we can fix their problems. Professor Doctor Coşkun Yıldız often quotes a phrase “Healthy gum tissue is like a ‘frame’ for the picture.” If that frame gets irritated very much by the rough edge of the veneer, the gums become swollen, bleed and start to smell.
Composite vs. Porcelain: Material Matters
We can’t say they are the same. We see a huge difference in the quantity of odor that the veneer is capable of holding.
Composite veneers (which are usually less expensive) are composed of resin. Imagine resin being like a plastic container that you keep your food in, a Tupperware. Over time it can develop small scratches. These scratches can then accumulate stains and odors.
Porcelain, which is our main focus here in Turkey, can be compared to a glass plate. It is completely resistant. You can spill a cup of coffee, perfume, curry or wine on it, when you rinse it, it will be completely clean. It does not retain odors.

Comparison: Risk Factors for Odor
| Feature | Composite Resin Veneers | Cheap/Poorly Fitted Porcelain | Lema Precision Porcelain |
| Porosity | High (Absorbs fluids over time) | Low (Material is good, fit is bad) | Zero (Glass-like surface) |
| Fit Accuracy | Variable | Poor (Creates “Ledges”) | Micro-Precision |
| Bacteria Trap | High (Surface scratches easily) | High (Trapped at gumline) | None (Seamless bonding) |
| Long-Term Odor | Common after 2-3 years | Immediate if hygiene fails | Rare to Non-Existent |
How We Prevent “Veneer Breath” in Turkey
When you sit in the chair with Dentist Polen Akkılıç, the focus isn’t just on how white the teeth are. It is on the emergence profile.
This is a technical term for how the tooth comes out of the gum. It needs to be a smooth, natural slope. Any thick or bulky piece of it will trap food. Hence, we are using digital scanning and 3D designing to make sure that the veneer will be perfectly fitted and closely stuck onto the tooth, so the tooth is completely sealed off from bacteria.
FAQ: Your Questions Answered by the Experts
Absolutely. If you have older veneers and are noticing a smell, a water flosser is your best defense until you can see a dentist. It shoots a pressurized stream of water that can sometimes penetrate those “ledges” we talked about earlier. However, this is a management tool, not a cure. If there is a gap, it eventually needs to be closed professionally.
Generally, no. Modern dental bonding agents are inert. However, if the bonding fails and saliva leaks underneath the veneer (we call this “micro-leakage”), the tooth underneath can start to decay. That distinct “rotten” smell is actually the underlying tooth suffering, not the glue itself.
It is possible to have a temporary metallic taste or slight scent during the first few days of healing, especially if there was minor gum contouring involved. This is just the tissue healing—similar to a scab on your knee. We prescribe a special chlorhexidine mouthwash to keep the area sterile and fresh during this short recovery window.
Morning breath is normal for everyone because saliva production drops while you sleep. Saliva is nature’s mouthwash. With veneers, if you have any plaque retention areas, the bacteria have 8 hours of dry conditions to multiply without being washed away. Drinking water immediately upon waking and scraping your tongue can help significantly.
We advise against relying on alcohol-based mouthwashes to mask the problem. Alcohol dries out the mouth, which actually encourages bacteria growth in the long run. If the smell is persistent, it’s a red flag that there is a biological issue—either a gap in the veneer or gum disease—that requires a dentist’s eye, not just minty liquid.
- Al-Maweri, S. A., et al. (2020). Efficacy of water flossing on clinical parameters of inflammation and plaque: A systematic review and meta-analysis. International Journal of Dental Hygiene, 18(2), 126-140.
- Bollen, C. M. L., & Bebler, J. (2020). Halitosis: the multidisciplinary approach. International Journal of Oral Science, 4(2), 55-63.
- Gurel, G., (2003). The Science and Art of Porcelain Laminate Veneers. Quintessence Publishing.
- Magne, P., & Belser, U. (2022). Bonded Porcelain Restorations in the Anterior Dentition: A Biomimetic Approach. Quintessence Publishing.
- Peumans, M., et al. (2018). Clinical effectiveness of contemporary adhesives: A systematic review of current clinical trials. Dental Materials, 34(11), 1637-1650.

