
Safe professional scaling and hygiene.
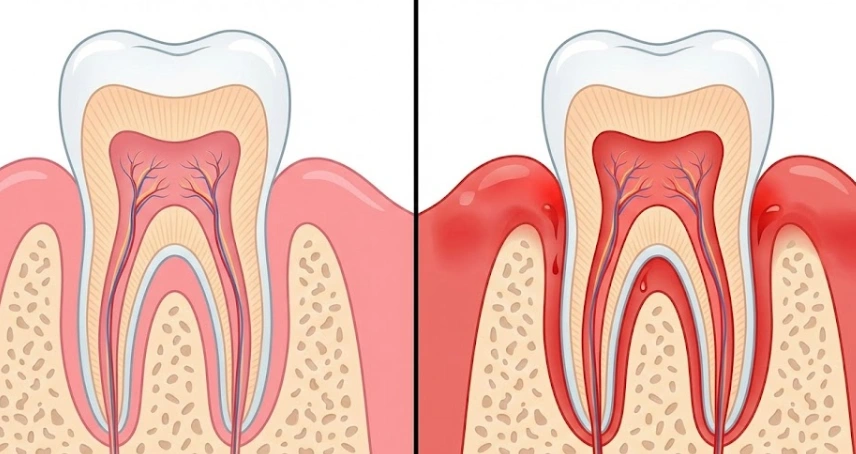
One of the wonderful things about pregnancy is a complete overhaul of your life plan, from painting the nursery, picking up names, to a roller-coaster of emotions. What women don’t expect, and yet, some of them get scared when the foam at the mouth after teeth brushing in the morning is pink. And if your gums are tender, swollen, and even bleeding, then you probably have “pregnancy gingivitis.“
Basically, your body is giving the babe most of the resources, and your gums become ultra-sensitive to the tiniest bacteria by literally the huge increase in progesterone. In short, if your gums are the soil, then during pregnancy, the soil becomes loose and you get a bigger reaction anytime. The slightest plaque that a year ago wouldn’t have been any problem can now blow up into a massive inflammatory response.
In our clinical experience at Lema Dental Clinic, this is something that we have witnessed live very often. Women who are expecting come before us in Turkey and are so scared that a dental treatment can be somehow harmful to their baby. We are here to tell you – the real risk is that you are ignoring the infection.
The “Why” Behind the Bleeding
It’s not just about brushing harder. The hormonal shifts alter your body’s immune response. Professor Doctor Coşkun Yıldız frequently explains to our patients that this hormonal tide can sometimes lead to localized swellings known as “pregnancy tumors” (pyogenic granulomas). Don’t let the scary name fool you—these are non-cancerous, raspberry-like bumps that usually fade after delivery. However, they are a loud signal from your body that your oral hygiene needs a professional assist.
Simple gingivitis, if left untreated, can definitely lead to periodontitis, which affects the jawbone that holds your teeth in place. It’s similar to finding out that the base of your house is deteriorating while you are occupied with decorating the room upstairs.
Safe Treatment Pathways in Turkey
The question remains: When is it safe to sit in the dentist’s chair?
At Lema Dental Clinic, we operate on a strict safety protocol. Dentist Polen Akkılıç and her team generally recommend scheduling non-emergency treatments during the second trimester. This is the “sweet spot”—the critical organ development of the first trimester is complete, and the physical discomfort of the third trimester hasn’t set in yet.
Here is how we tackle it:
- Ultrasonic Scaling: We use high-tech vibrations to gently vibrate the tartar “barnacles” off your teeth. This removes the bacterial load without invasive surgery.
- Root Planing: If the pockets around your teeth are deep, we smooth the root surfaces. Imagine sanding a rough piece of wood so that the varnish (your gums) can adhere smoothly again.
- Chlorhexidine Rinses: We may prescribe specialized alcohol-free mouthwashes to keep the bacterial count low between visits.

Comparing Treatment Windows
Navigating dental care while pregnant requires timing. Here is a breakdown of how we manage treatments across the trimesters at our clinic:
| Trimester | Timing | Recommended Action | Risk Level |
| First (Weeks 1-13) | Baby’s organs forming | Emergency Only. Stick to plaque control and exams. Avoid X-rays unless critical. | High (due to organogenesis) |
| Second (Weeks 14-27) | The “Safe Zone” | Ideal time for treatment. Scaling, root planing, and routine fillings are safe. | Low (Best window for care) |
| Third (Weeks 28-40) | Baby growing rapidly | Comfort focus. Short appointments to avoid back pain. Treat only if necessary to prevent infection. | Low-Moderate (Discomfort risk) |
Common Questions About Pregnancy Dental Care
Not at all. The local anesthetics we use, like Lidocaine, are considered Category B drugs, meaning they are safe for you and the baby. We use the minimum effective dose to ensure you are pain-free without affecting your little one.
We strongly advise against waiting if you have active infection. Studies have shown a link between untreated gum disease and preterm birth or low birth weight. Treating your gums is actually part of prenatal care.
Yes, with modern precautions. At Lema Dental Clinic, if an X-ray is absolutely necessary, we use a leaded apron and thyroid collar to shield you and the baby completely. However, for gum disease, we often don’t even need X-rays to start treatment.
It feels counterintuitive, but bleeding means you need to clean more, not less. The bleeding is the infection leaving the body. Keep flossing gently; the bleeding will stop once the inflammation subsides.
Don’t panic. If it’s not painful or interfering with chewing, we usually leave it alone and it disappears after birth. If it bleeds excessively or bothers you, Professor Doctor Coşkun Yıldız can remove it safely with a quick, minor procedure.
- Cobb, C. M., Kelly, P. J., Williams, K. B., Babbar, S., Angolkar, M., & Derman, R. J. (2017). The oral microbiome and adverse pregnancy outcomes. International Journal of Women’s Health, 9, 551–559.
- Figuero, E., Han, Y. W., & Furuya, Y. (2020). Periodontal therapy for the prevention of adverse pregnancy outcomes: A clinically focused review. Periodontology 2000, 83(1), 164–182.
- Jang, H., Patoine, A., Wu, T., Castillo, D. A., & Xiao, J. (2021). Oral microflora and pregnancy: A systematic review and meta-analysis. Scientific Reports, 11(1), 16870.
- Offenbacher, S., Beck, J. D., Jared, H. L., Mauriello, S. M., Mendoza, L. C., Couper, D. J., … & Murtha, A. P. (2009). Effects of periodontal therapy on rate of preterm delivery: A randomized controlled trial. Obstetrics & Gynecology, 114(3), 551–559.
- Sanz, M., Kornman, K., & Working Group 3 of the Joint EFP/AAP Workshop. (2013). Periodontitis and adverse pregnancy outcomes: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. Journal of Clinical Periodontology, 40(s14), S164–S169.

