
Abstract: The ultimate manual dives into Dental Code D7952, elaborating on a biologically guided, one-sided surgical intervention called vertical approach sinus augmentation, with the focus narrowed down to the least invasive side of the surgical procedure, less anatomical involvement, and consequently less patient discomfort. This compendium intends to clarify the pathway to how this innovative technique allows dental implant placement in the atrophic posterior maxilla with the help of clear visuals and lucid explanations. This resource is designed for patients and dental professionals seeking a clear, accurate understanding of how this advanced method facilitates dental implant placement in the atrophic posterior maxilla.
Overcoming the Challenge of the Posterior Maxilla

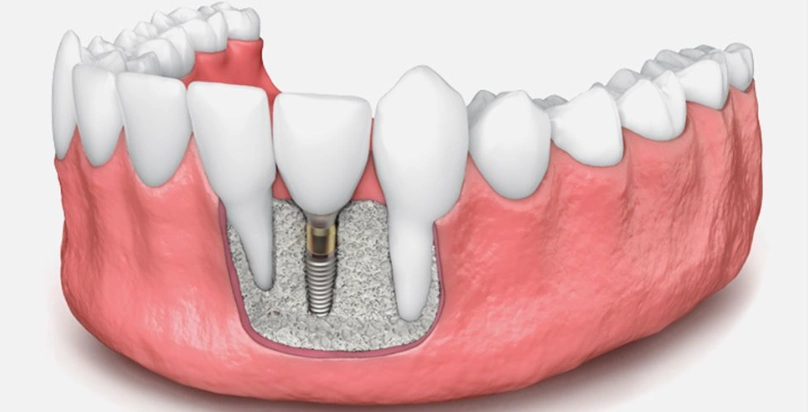
Implant procurement of the dentition is dependent on two major factors: enough volume and density of the living jawbone must be present. Now, the posterior upper jaw or the posterior maxilla, as they say, is quite a challenging anatomical area for a dentist and a patient. This is the region that undergoes almost double the amount of bone loss it did before tooth loss. And, pneumatization of the maxillary sinus is a second critical factor that complicates implant dentistry in the region further.
The maxillary sinus is an air-filled space located between the roots of the upper back teeth. After tooth extraction, this sinus goes through its natural expansion, a procedure called pneumatization. Such enlargement concurrently reduces the bone height available between the oral cavity and the sinus floor. Medical professionals refer to this state as sub-sinus bone height deficiency. When bone height is less than 8-10 mm, which is the standard for implant stability, surgical intervention is the only way out.
Dental Code D7952 is an example of a complex operation that includes vertical approach sinus augmentation. This action neutralizes the challenge of a lack of bone height by going up the sinus membrane and grafting bone there to have a stable support for the dental implant’s success.
Defining Dental Code D7952: Precision in Terminology
According to the American Dental Association (ADA) Current Dental Terminology (CDT) code, D7952 is a detailed description of “sinus augmentation via a vertical approach.”
The particular term helps to understand the operation concept in comparison with the common way, D7951 (sinus augmentation via a lateral window approach). The main difference is in the surgical access point. With the vertical method, accessing the sinus cavity is done through the alveolar ridge crest, the gum tissue at the site of the missing tooth. Clinically, the technique is also termed Osteotome-Mediated Sinus Floor Elevation (OMSFE) or the Crestal Approach Sinus Lift.
The goal of the operation is to carefully lift the Schneiderian membrane (the sinus lining) through the dental implant opening, thus creating a space under it. The bone graft is then introduced to this new space, thus the sinus floor is effectively raised and vertical bone height is increased.
Primary Indications: When is the Vertical Approach the Optimal Choice?

Dental professionals decide upon a recommendation of the D7952 technique after careful consideration of the clinic-based measurable factors. It is not a universal manner, but very effective for certain well-defined cases.
The main indication for a vertical sinus floor lift is a slightly to moderately sub-sinus bone height with speculation. Typically, this means an existing bone height of 4 mm to 8 mm. Within this interval, the vertical approach offers the closest and the least traumatic way of finding the last 3-6 mm of bone essential for dental implant positioning.
Important patient factors that support the vertical approach are:
- Need for a Less Invasive Procedure: The crestal access is a reason for less postoperative swelling and pain compared with the lateral window technique.
- Simultaneous Implant Placement: In many situations with 4-5 mm of initial bone, dentists can do the dental implant placement right after the sinus augmentation in a single surgical session.
- Preservation of Anatomical Structures: The method does not necessitate the manipulation of the lateral sinus wall, thus less probability of blood vessels and nerves in that area.
- Managing Narrow Ridges: The method is especially beneficial if the jawbone ridge is too slim for a lateral window without structural integrity loss.
4The Surgical Protocol: A Step-by-Step Overview
The operation phases explanation clears up the surgical precision and the practitioner’s tricks. It follows the ordered steps of the vertical sinus augmentation.
Step 1: Comprehensive Pre-Surgical Planning
The oral surgeon makes a 3D Cone Beam Computed Tomography (CBCT) scan as the first step. This high-tech imaging reveals a very detailed, three-dimensional view of the sinus anatomy, the membrane thickness, the bone volume, and the absolute location of the vital parts. The CBCT figures are the main reason for deciding the correct sizes of osteotomes and the implant path.
Step 2: Local Anesthesia and Flap Reflection
Local anesthesia and flap reflection make the patient totally comfortable. The surgeon administers local anesthesia. Next, a minor incision is performed along the alveolar ridge crest, and the gum tissue is carefully lifted to uncover the bone underneath at the place where the implant will be fitted.
Step 3: Sequential Bone Preparation
The surgeon accomplishes a precise osteotomy (pilot hole) at the site of implant. The surgeon then readies the bone. Through a set of specialized concaved-end tools, namely osteotomes, a surgeon gradually punches the bone laterally and apically. This consecutive operation does not extract the bone; on the contrary, it densifies it, thus the implant stability is enhanced without any threat to the primary fixation.
Step 4: Sinus Membrane Elevation
Before the sinus floor arrival, controlled hammering is used to break the very thin bone of the sinus floor, thus creating a greenstick fracture, while at the same time, the osteotome tip disengages and gently moves the Schneiderian membrane up, thus forming a tent-like space. Surgeons often use the Valsalva maneuver to check the integrity of the membrane at this moment.
Step 5: Graft Material The surgeon
This implant is introduced by the surgeon very delicately through the osteotomy site in the space under the lifted membrane. This bone graft will not only hold the membrane but will also stimulate the body to send its own cells for the formation of new, living bone, which will take place between 4-9 months.
Step 6: Implant Placement and Closure
If there is enough primary stability of the bone, the dentist will go on with the immediate implant insertion into the grafted area. At last, the surgeon closes the operation by sewing the gum tissue back in place.
| Feature | D7952: Vertical Approach | D7951: Lateral Window Approach |
|---|---|---|
| Surgical Access | Through the crest of the ridge (minimally invasive) | Through a window cut into the lateral sinus wall (more invasive) |
| Ideal Bone Height | 4 mm – 8 mm | Less than 4 mm – 5 mm |
| Implant Timing | Often simultaneous | Almost always staged (implant placed 6-9 months later) |
| Visualization | Limited, “blind” technique | Direct visualization of the sinus membrane |
| Primary Advantage | Minimal morbidity, shorter surgery time | Ability to address severe bone deficiencies |
| Primary Risk | Higher risk of membrane perforation in less experienced hands | Longer healing time, more postoperative discomfort |
D7952 vs. D7951: A Comparative Analysis
The decision to use vertical (D7952) or lateral (D7951) methods depends on a careful clinical examination of anatomical structures.
The Crucial Function of Bone Grafting Materials
The bone graft implanted in a D7952 operation is what makes the fusion successful. The implant material performs three vital tasks:
- It physically supports the raised sinus membrane.
- It constructs a framework, or matrix, that directs the new bone growth.
- It offers a source of osteoinductive and osteoconductive factors that activate the body’s natural healing process.
- Autografts: The patient’s own bone, which is the best source, but it necessitates an extra surgical site.
- Allografts: A freeze-dried bone from one donor, a single source, taken from a certified tissue bank, is a very effective and thus a widely used option.
- Xenografts: Bovine (cow) bone mineral, which can provide a good long-term scaffold.
- Alloplasts: Artificial bone substitute materials, e.g., hydroxyapatite or beta-tricalcium phosphate.
The surgeon will decide the best graft material for you according to your biological needs and the clinical goals of the surgery.
The Recovery and Healing Process: What to Expect
Postoperative care is simple and vital for the achievement of the best result. Patients should expect a fast recovery with a little bit of discomfort.
Immediate Postoperative Period (First 24-48 Hours):
- Help the anti-inflammatory (medicine prescribed or over-the-counter) to relieve minor swelling and discomfort.
- Put ice on the cheek near the surgical site for 15-minute intervals and remove it for an equal period of time.
- Keep to a soft food diet and do not consume hot liquids.
- Don’t blow your nose, sneeze with your mouth open, spit icing or use a straw as these actions can cause pressure that can lead to the disruption of the healing graft.
First Week and Beyond:
- Keep up with the oral hygiene routine but be gentle at the same time, clean the area around the surgical site as instructed.
- Go to all the follow-up visits scheduled for you so that your healing process can be checked.
- Usually, the bone graft can be considered mature from 4 to 9 months and then the implant can be restored with a crown if it was not placed immediately.
Evaluating Success Rates and Possible Risks
Vertical sinus augmentation shows high long-term success rates, as single clinical trials report it to be at over 95% for implant survival when an experienced clinician performs the operation on the right patients.
Knowing the possible risks is part of the process of giving informed consent, which is necessary before any operation. The commonest risk is perforation of the Schneiderian membrane. If a small hole shouldn’t have any effect on the result whereas if the hole is larger, then it will be necessary to repair it or change the lateral approach. A few other risks that are seldom considered are infection, graft migration, and sinusitis. The probabilities for these events are small and your surgeon uses strict sterile techniques and accurate planning to overcome them effectively.
A Predictable Path to Restorative Success

Dental Code D7952, which is a sinus augmentation through a vertical approach, is a major implant dentistry innovation. It gives a very predictable, minimally invasive, patient-friendly way of doing the trick to get enough bone height in the difficult posterior maxilla. Hence, besides reshaping the face by replacing stable, long-lasting dental implants, the operation brings back not only the lost chewing function and oral health but the overall quality of life as well. If your dentist has mentioned that there is not enough bone to support an implant, the next thing to do is to see a specialist experienced with the D7952 method, who will let you know if this accurate and efficient procedure is the way to your oral rehabilitation.
References
- Jensen, O. T. (Ed.). (2019). The Sinus Bone Graft (3rd ed.). Quintessence Publishing. (A foundational textbook covering all sinus lift techniques).
- Sharan, A., & Madjar, D. (2008). Maxillary sinus pneumatization following extractions: a radiographic study. International Journal of Oral & Maxillofacial Implants, 23(1), 48-56. (Documents the phenomenon of sinus expansion post-tooth loss).
- Pjetursson, B. E., & Lang, N. P. (2014). Sinus floor elevation utilizing the transalveolar approach. Periodontology 2000, 66(1), 59-71. (A comprehensive review article on the crestal approach, including indications and protocols).
- Summers, R. B. (1994). A new concept in maxillary implant surgery: The osteotome technique. Compendium, 15(2), 152-162. (The seminal paper that introduced the osteotome technique).
- Tan, W. C., Lang, N. P., Zwahlen, M., & Pjetursson, B. E. (2013). A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. Part II: Transalveolar technique. Journal of Clinical Periodontology, 40(Suppl 14), S156–S171. (A key systematic review confirming high success rates for the vertical approach).
Frequently Asked Questions (FAQs) About Dental Code D7952
The core difference is the surgical access point. D7952 (Vertical/Crestal Approach) is minimally invasive, performed through the gum where the implant will be placed. D7951 (Lateral Window Approach) involves creating a window in the side of the gum and cheekbone to access the sinus, making it a more extensive procedure.
Ideal candidates have a moderate lack of bone height under the sinus, typically between 4mm and 8mm. This procedure is also excellent for patients seeking a less invasive option with potentially quicker recovery and for cases where an implant can be placed immediately.
Yes, the D7952 procedure is typically performed under local anesthesia, ensuring the area is completely numb and the patient feels no pain. Sedation options may also be available for anxious patients, which should be discussed with your surgeon beforehand.
Yes, in many cases, the dental implant can be placed immediately following the sinus augmentation in a single surgical session. This simultaneous approach depends on achieving sufficient initial stability from the remaining bone, which your surgeon will assess with a 3D CBCT scan.
Surgeons use thoroughly processed and sterilized bone graft materials from human (allograft), animal (xenograft), or synthetic (alloplast) sources. All graft materials used in the U.S. are regulated by the FDA and/or the American Association of Tissue Banks (AATB), ensuring they are safe, biocompatible, and free from disease transmission.
When performed on appropriately selected patients, the procedure has a very high long-term success rate, with clinical studies consistently reporting implant survival rates of over 95% after the bone has healed and integrated with the implant.


